Your doctor may recommend knee replacement surgery if you have severe knee pain and disability from rheumatoid arthritis, osteoarthritis, or traumatic injury. A knee replacement can relieve pain and help you live a fuller, more active life.
The surgeon will replace your damaged knee with an artificial device (implant). Although the total knee joint replacement is the more preferred procedure, some people can benefit from just a partial knee replacement.
Implants are made of metal alloys, and strong plastic parts, and can be joined to your bone by acrylic cement. There are many different types of implants. Discuss with your surgeon which implant is best for you.

Your knee is the largest and strongest joint in your body. The knee joint is where the lower end of your femur (thighbone) meets the upper end of your tibia (shinbone). Your patella (kneecap) sits in front of the joint to provide some protection.
A healthy knee lets you move your lower leg forward and backward, and swivel slightly to point your toes in or out. Ligaments and cartilage stabilize and support the joint, preventing your knee from moving too far from side to side.
Types of DesignsFor simplicity, the knee is considered a "hinge" joint because of its ability to bend and straighten like a hinged door. In reality, the knee is much more complex because the bone surfaces actually roll and glide as the knee bends.
The first implant designs used the hinge concept and included a connecting hinge between the parts. Newer implant designs recognize the complexity of the joint and more closely mimic the motion of a normal knee. Some designs preserve the patient's own ligaments, while others substitute for them.
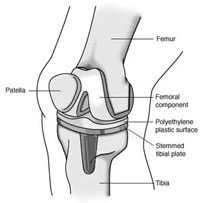 Knee implant components
Knee implant components
Up to three bone surfaces may be replaced in a total knee replacement
 Posterior-stabilized component.
Posterior-stabilized component.
Components are designed so that metal always adjoins with plastic, which provides smooth movement and results in minimal wear.
In these designs, the cushion of the tibial component has a raised surface with an internal post that fits into a special bar (called a cam) in the femoral component. The posterior cruciate ligament is removed to fit the components to the bone. The pieces work together to do what the posterior cruciate ligament does: prevent the thighbone from sliding forward too far on the shinbone when you bend your knee.
 Cruciate-retaining component.
Cruciate-retaining component.
As the name implies, the posterior cruciate ligament is kept with this implant design. Cruciate-retaining implants do not have the center post and cam design. This implant may be appropriate for a patient whose posterior cruciate ligament is healthy enough to continue stabilizing the knee joint.
In total knee replacement, large implants are used to resurface the ends of the femur and tibia. If only one side of the knee joint is damaged, smaller implants can be used (unicompartmental knee replacement) to resurface just that side.
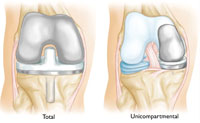
In a unicompartmental (partial) knee replacement, only the damaged part of the knee is replaced.
Fixed- vs. Mobile-Bearing Prosthesis (Implant)Most patients get a fixed-bearing prosthesis. In this design, the polyethylene of the tibial component is attached firmly to the metal implant beneath. The femoral component then rolls on this cushioned surface.
In some cases, excessive activity and/or extra weight can cause a fixed-bearing prosthesis to wear down more quickly. Worn components can loosen from the bone and cause pain. Loosening is a major reason some artificial joints fail.
If you are younger, more active, and/or overweight, your doctor may recommend a rotating platform/mobile-bearing knee replacement. These implants are designed for potentially longer performance with less wear.
Like fixed-bearing implants, mobile-bearing implants use three components to provide a relatively natural joint. In a mobile-bearing knee, however, the polyethylene insert can rotate short distances inside the metal tibial tray.
This is designed to allow patients a few degrees of greater rotation to the medial and lateral sides of their knee.
Compared with fixed-bearing designs, mobile-bearing knee implants require more support from soft tissues, such as the ligaments surrounding the knee. If the soft tissues are not strong enough, mobile-bearing knees are more likely to dislocate. They also may cost more than fixed-bearing implants.
Implant MaterialsThe metal parts of the implant are made of titanium or cobalt-chromium based alloys. The plastic parts are made of ultra high molecular weight polyethylene.
The longevity and performance of a knee replacement depends on several factors, including your activity level, weight, and general health.
Just as wear in the natural joint contributed to the need for a replacement, wear in the implant may eventually require a second surgery (called a joint revision).
Revision surgery may require special components. Typically they will have longer stems which fit into the femur and tibia. They may also have attached metal pieces called augments which substitute for missing bone.
Revision components often have a cam in the center of the knee similar to a posterior stabilized component. In revision components, though, the cam is larger to give the knee more stability.
In cases where the knee is very unstable and a large amount of bone is missing, it may be necessary to join the femur and tibia with a metal "hinge" in the center.
Total hip joint replacement is an orthopaedic success story. There have been many advances in the design, construction, and implantation of artificial hip joints, resulting in a high percentage of successful long-term outcomes.
Implant DesignThe hip joint is called a ball-and-socket joint because the spherical head of the thighbone (femur) moves inside the cup-shaped hollow socket (acetabulum) of the pelvis.
To duplicate this action, a total hip replacement implant has three parts: the stem, which fits into the femur; the ball, which replaces the spherical head of the femur; and the cup, which replaces the worn out hip socket.
The brand, performance & cost issues you may discuss with doctor.
Today, the stem portions of most hip implants are made of titanium- or cobalt/chromium-based alloys. They come in different shapes and some have porous surfaces to allow for bone ingrowth.
Cobalt/chromium-based alloys or ceramic materials (aluminum oxide or zirconium oxide) are used in making the ball portions, which are polished smooth to allow easy rotation within the prosthetic socket.
The acetabular socket can be made of metal, ultra-high molecular-weight polyethylene, or a combination of polyethylene backed by metal.
All the materials used in a total hip replacement have four characteristics in common:
Cemented Total Hip Replacement
Over the past 40 years, there have been many improvements in both the materials and the methods used to hold the femoral and acetabular components in place. Today, the most commonly used bone cement is an acrylic polymer called polymethylmethacrylate (PMMA).
A patient with a cemented total hip replacement can put full weight on the limb and walk without support almost immediately after surgery, resulting in a faster rehabilitation. Although cemented implants have a long and distinguished track record of success, they are not considered.
Cemented fixation relies on a stable interface between the prosthesis and the cement and a solid mechanical bond between the cement and the bone. Today's metal alloy stems rarely break, but they can occasionally loosen. Two processes, one mechanical and one biological, can contribute to loosening. Cracks in the cement can cause the prosthetic stem to loosen & become unstable.
Despite these recognized failure mechanisms, the bond between cement and bone is generally very durable and reliable. Cemented total hip replacement is more commonly recommended for older patients, for patients with conditions such as rheumatoid arthritis, and for younger patients with compromised health or poor bone quality and density. These patients are less likely to put stresses on the cement that could lead to fatigue fractures.
Cementless Total Hip ReplacementNew implant designs are now available since last so many years which attach directly to bone without the use of cement.
They also have a surface topography that is conducive to attracting new bone growth. Most are textured or have a surface coating around much of the implant so that the new bone actually grows into the surface of the implant. Because they depend on new bone growth for stability, cementless implants require a longer healing time than cemented replacements.
The orthopaedic surgeon must be very precise in preparing the femur for a cementless impact. The implant channel must match the shape of the implant itself very closely. New bone growth cannot bridge gaps larger than 1 mm to 2 mm.
Your surgeon may recommend a period of protected weight-bearing (using crutches or a walker) to give the bone time to attach itself to the implant. This protected weight bearing helps to ensure there is no movement between the implant and bone so a durable connection can be established.
Cementless femoral components tend to be much larger at the top, with more of a wedge shape. This design enables the strong surface (cortex) of the bone and the dense, hard spongy (cancellous) bone just below it to provide support.
The acetabular component of a cementless total hip replacement also has a coated or textured surface to encourage bone growth into the surface. Depending on the design, these components may also use screws through the cup or spikes, pegs, or fins around the rim to help hold the implant in place until the new bone forms. Usually these components have a metal outer shell and a polyethylene liner.
The pelvis is prepared for a cementless acetabular component using a process similar to that used in a cemented total hip replacement procedure. The intimate contact between the component and bone is crucial to permit bone in growth.
Initially, it was hoped that cementless total hip replacement would eliminate the problem of bone resorption or stem loosening caused by cement failure. Although certain cementless stem designs have excellent long-term outcomes, cementless stems can loosen if a strong bond between bone and stem is not achieved.
Patients with large cementless stems may also experience a higher incidence of mild thigh pain. Likewise, polyethylene wear, particulate debris, and the resulting osteolysis (dissolution of bone) remain problems in both cemented and uncemented designs. Improvements in the wear characteristics of newer polyethylene, and research into newer bearing surfaces may help resolve some of these problems in the future.
Although some orthopaedic surgeons are now using cementless devices for all patients, cementless total hip replacement is most often recommended for younger, more active patients and patients with good bone quality where bone ingrowth into the components can be predictably achieved. Individuals with juvenile inflammatory arthritis may also be candidates, even though the disease may restrict their activities.
A hybrid total hip replacement has one component, usually the acetabular socket, inserted without cement, and the other component, usually the femoral stem, inserted with cement.
Partial Hip ReplacementsIf only one part of the joint is damaged or diseased, a partial hip replacement may be recommended. In most instances, the acetabulum is left intact and the head of the femur is replaced, using components similar to those used in a total hip replacement. The most common form of partial hip replacement is called a bipolar prosthesis.
Hip ResurfacingA newer technique for hip replacement that has recently emerged is called hip resurfacing. In this procedure, the socket is replaced similar to a total hip replacement. The femur, however, is covered or "resurfaced" with a hemispherical component. This fits over the head of the femur and spares the bone of the femoral head and the femoral neck. It is fixed to the femur with cement around the femoral head and has a short stem that passes into the femoral neck.
Hip resurfacing is an emerging procedure, most commonly performed in younger patients. It is too early to assess the long-term success of this procedure.
Longevity and OutcomesHip replacement operations are highly successful in relieving pain and restoring movement. However, the ongoing problems with wear and particulate debris may eventually necessitate further surgery, including replacing the prosthesis (revision surgery). Men and patients who weigh more than 165 lb have higher rates of failure. The chance of a hip replacement lasting 20 years is approximately 80%.
 +91 9873114480,
9810894321
+91 9873114480,
9810894321






